

If you’re looking for the best spectacles for myopia in children, consider highly aspherical lenslets (HAL) or DIMS lenses. Research shows that spectacles for myopia with HAL lenses can slow myopia progression by up to 0.80 diopters and reduce axial length growth by 0.35 mm over two years. DIMS spectacles for myopia also decrease axial elongation by 62% compared to standard lenses. Executive bifocals are another option, especially effective for younger children. Using spectacles for myopia is crucial for controlling myopia, protecting your child’s eye health, and reducing the risk of serious vision issues. With this information, you can confidently choose the right spectacles for myopia to manage your child’s condition.
Quick Comparison Table:
Lens Type
Myopia Progression Slowing
Axial Length Reduction
HAL
0.80 D
0.35 mm
DIMS
~0.4 D
~0.3 mm
Executive Bifocals
0.75 D
0.25 mm
Key Takeaways
Spectacle lenses with highly aspherical lenslets (HAL) and DIMS lenses are the most effective at slowing myopia progression and eye growth in children.
Early myopia control helps reduce the risk of serious eye problems later in life and improves your child’s long-term vision health.
Choosing the right spectacles depends on your child’s age, myopia severity, and vision needs; consulting an eye care professional is essential.
Consistent use of myopia control spectacles, combined with healthy habits like outdoor play, supports better treatment outcomes.
Regular eye exams every six months help track progress and ensure the chosen treatment works well for your child.
Best Lenses
Top Choices for Myopia Control
When you look for the most effective myopia control treatments for your child, you want clear answers. Recent research highlights several spectacle lenses and other treatment options that stand out for myopic children. Here are the top choices:
Highly Aspherical Lenslets (HAL): These spectacle lenses use a special design to slow myopia progression. Studies show HAL lenses can reduce myopia progression by up to 0.80 diopters and axial length growth by 0.35 mm over two years. This makes them one of the most effective spectacle lenses for myopia control.
DIMS Spectacle Lenses: DIMS lenses use a unique lenslet pattern to create myopic defocus. They slow axial elongation by about 0.34 mm and reduce myopia progression by 0.44 diopters. DIMS lenses work well for children from different backgrounds and have shown consistent results in both UK and Chinese populations.
Executive Bifocals: These spectacle lenses split the lens into two parts, helping to control myopia in children, especially those aged 8 to 13. Executive bifocals can slow myopia progression by about 0.75 diopters and reduce axial length growth by 0.25 mm over two years.
MiSight Contact Lenses: Although not spectacles for myopia, MiSight lenses are FDA-approved and offer strong myopia control. They slow progression by 0.66 diopters and axial elongation by 0.28 mm.
Orthokeratology Lenses: These lenses reshape the cornea overnight. They are not spectacle lenses, but they provide another option for myopic children who need effective myopia control treatments.
Low-Dose Atropine: This eye drop is not a lens, but it is often used alongside spectacle lenses or contact lenses for myopia control. Atropine 0.05% can reduce myopia progression by 0.54 diopters and axial length by 0.21 mm.
Tip: You should always discuss these treatment options with your eye care professional to find the best fit for your child’s needs.
Key Study Findings
Researchers have compared many spectacle lenses and other interventions to find the best ways to slow myopia in children. The most reliable studies use randomized controlled trials, focus on axial length changes, and include children aged 6 to 12 years. Here are some important findings:
A 12-month study in Spain found that spectacle lenses with asymmetric myopic peripheral defocus (MPDL) reduced axial length growth by 37.3% compared to single vision lenses. The difference in axial length change was 0.09 mm over one year.
DIMS lenses reduced axial length progression by 0.21 mm, while HALT lenses reduced it by 0.23 mm. CARE and DOT lenses also showed positive effects, but to a lesser degree.
Meta-analyses show that HAL and DIMS spectacle lenses for myopia control provide the highest percentage reduction in myopia progression and axial elongation among spectacle-based treatments.
Lens Type |
Refraction Mean Difference (D) |
95% Confidence Interval |
Axial Length Mean Difference (mm) |
95% Confidence Interval |
Percentage Reduction in Myopia Progression |
Percentage Reduction in Axial Length Elongation |
|---|---|---|---|---|---|---|
Highly Aspherical Lenslets (HAL) |
0.80 |
0.77 – 0.83 |
-0.35 |
-0.36 to -0.34 |
67% |
64% |
MiSight Contact Lenses |
0.66 |
0.63 – 0.69 |
-0.28 |
-0.29 to -0.27 |
59% |
52% |
Low Dose Atropine 0.05% |
0.54 |
0.38 – 0.70 |
-0.21 |
-0.28 to -0.14 |
67% |
51% |
Biofinity +2.50 D Bifocal Lenses |
0.45 |
0.29 – 0.61 |
-0.24 |
-0.33 to -0.15 |
43% |
36% |
DIMS Spectacle Lenses |
0.44 |
0.42 – 0.46 |
-0.34 |
-0.35 to -0.33 |
87% |
61% |
Orthokeratology Lenses |
N/A |
N/A |
-0.24 |
-0.33 to -0.15 |
N/A |
N/A |
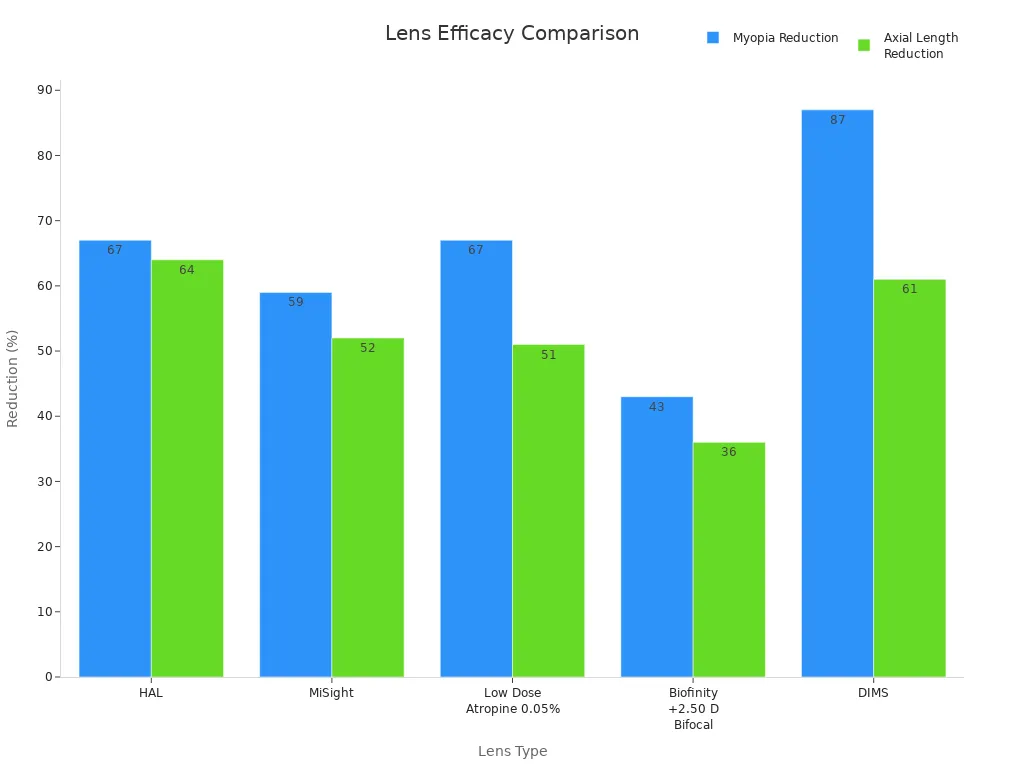
You can see from the table and chart that HAL and DIMS spectacle lenses for myopia control offer the highest two-year efficacy among spectacle-based options. MiSight contact lenses and low-dose atropine also provide strong results, but spectacle lenses remain the most accessible choice for many families.
Note: The best myopia control treatments show at least a 50% reduction in axial length progression compared to controls. HAL, DIMS, and executive bifocals meet this standard for myopic children.
When you choose spectacles for myopia, you want to know they work. The studies above show that modern spectacle lenses, especially HAL and DIMS, deliver strong treatment efficacy. These lenses help slow myopia progression and protect your child’s vision for the future.
Why Myopia Control Matters
Risks of Progressive Myopia
You need to understand the risks that come with progressive myopia in children. When myopia progression continues unchecked, it can lead to serious eye health problems later in life. As myopia increases, the risk of conditions like myopic macular degeneration, retinal detachment, and glaucoma rises sharply. For example, each extra diopter of myopia increases the risk of myopic maculopathy by 57%, open-angle glaucoma by 20%, and retinal detachment by 30%. These complications can cause permanent vision loss.
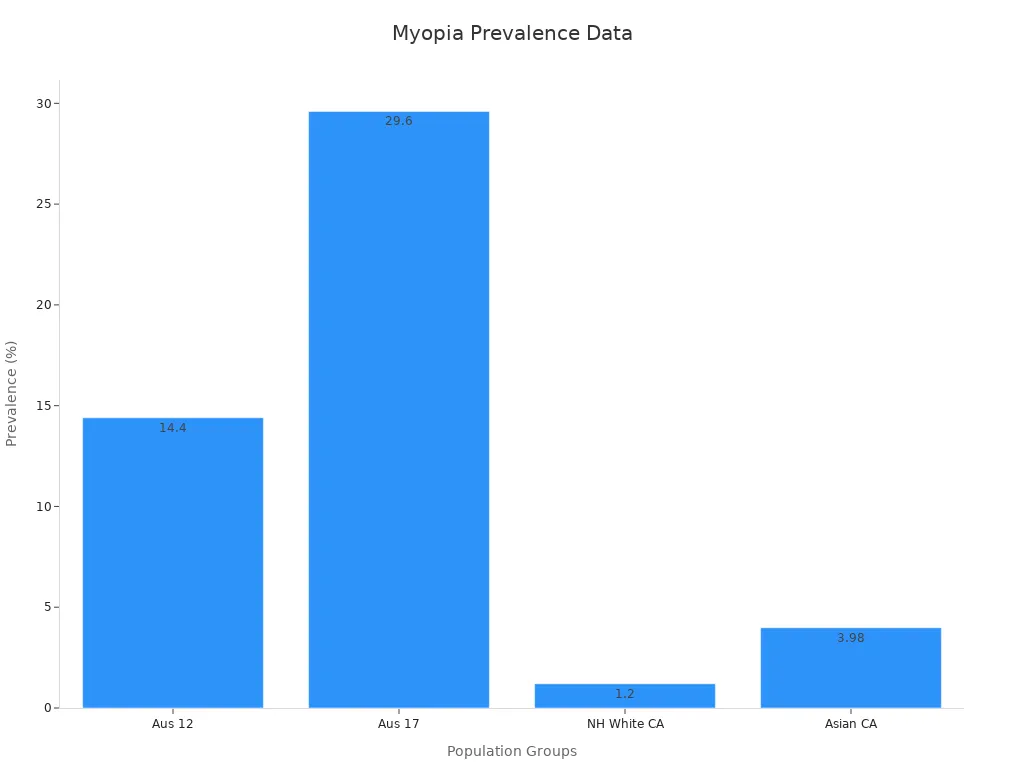
The prevalence of myopia is rising worldwide, especially in children from Asian populations, where up to 60% may develop myopia. In urban Asian communities, more than 14% of children develop new cases each year. In the United States and Western Europe, about one in four adults has myopia, and the rate has increased by 66% over the past 30 years. Children with two myopic parents face a risk more than six times higher than those with no myopic parents. The earlier myopia starts, the more years a child will experience progression, which leads to higher levels of myopia and greater risk of complications.
Note: Axial length growth in the eye is a key factor in myopia progression. Longer eyes are more likely to develop sight-threatening problems.
Benefits of Early Intervention
You can make a big difference by starting myopia control early. Early intervention slows myopia progression and reduces the risk of severe eye diseases in adulthood. Studies show that treating just four to seven children can prevent five years of visual impairment for one child. If you reduce myopia by even one diopter, you can lower the risk of vision loss and cut the years spent with visual impairment by up to 1.2 years for high myopes.
Children who receive myopia control treatments, such as special lenses or atropine drops, experience slower progression and less axial length growth. Comprehensive programs that include outdoor time, balanced screen use, and healthy sleep also help delay myopia progression. These steps protect your child’s vision and give them a better quality of life.
Metric |
Numerical Evidence |
|---|---|
Number needed to treat (NNT) to prevent 5 years of visual impairment |
|
Risk of vision loss due to myopia control treatment |
Fewer than 1 in 38 patients |
Reduction in years of visual impairment per 1 diopter reduction |
0.74–1.22 years |
🟢 Tip: Start myopia control as soon as possible. Early action means less progression and a lower chance of future eye problems.
Spectacles for Myopia Control

HAL Lenses
When you choose spectacle lenses with highly aspherical lenslets, you give your child one of the most effective myopia control treatments available. These lenses use a special design that creates zones of myopic defocus across the lens surface. This design helps slow myopia progression by signaling the eye to reduce its growth. In a five-year clinical study, children and adolescents wearing these lenses showed 1.75 diopters less myopia progression and 0.72 mm less axial length growth compared to standard single vision lenses. The risk of developing high myopia dropped from 38% to 9%. Spectacle lenses with highly aspherical lenslets work well for myopic children and adolescents, offering strong protection against future eye problems.
DIMS Lenses
DIMS spectacle lenses with highly aspherical lenslets also use myopic defocus to slow myopia progression. These lenses have a ring-shaped pattern of lenslets that create constant myopic defocus, which helps control eye growth. Studies show that DIMS lenses and HAL lenses have similar effects on myopia control. Over two years, both lens types slowed progression and axial length growth by about the same amount. In one study, 38.4% of children wearing DIMS lenses had no myopia progression after two years, compared to 21.9% with HAL lenses.
Parameter |
DIMS (Mean ± SD) |
HAL (Mean ± SD) |
Statistical Significance |
|---|---|---|---|
-0.50D (±0.64) |
-0.63D (±0.56) |
No significant difference |
|
2-year AL increase |
0.29 mm (±0.63) |
0.32 mm (±0.72) |
No significant difference |
Both DIMS and HAL spectacle lenses with highly aspherical lenslets offer excellent myopia control for myopic children and adolescents.
Executive Bifocals
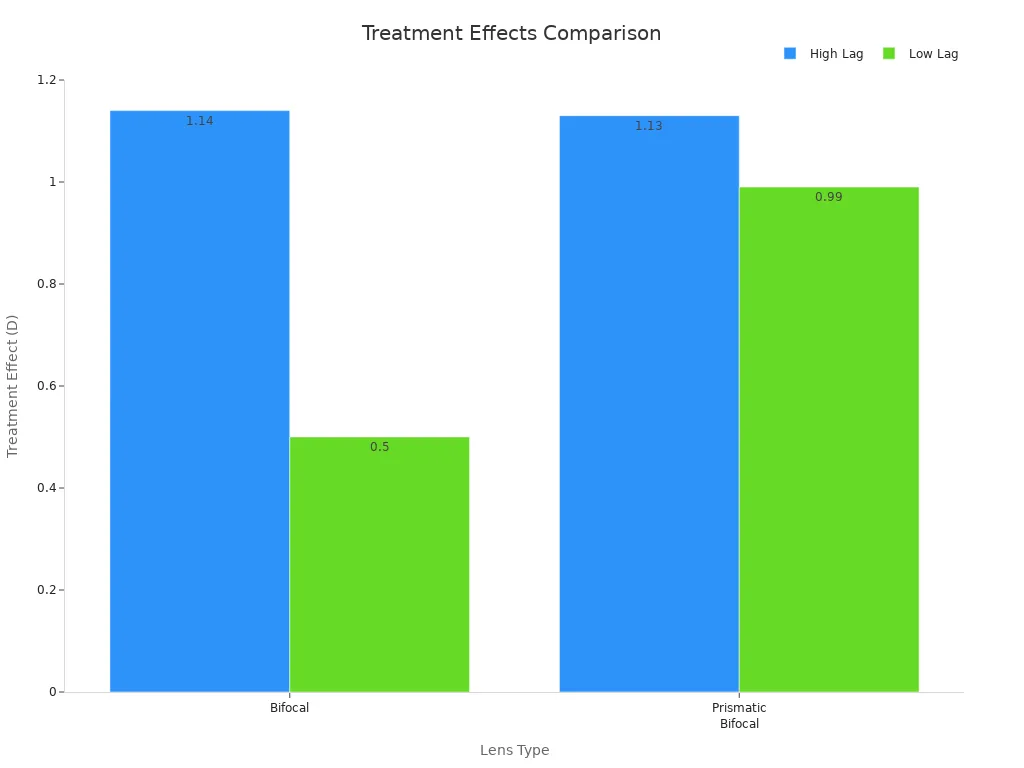
Executive bifocals split the lens into two clear zones: one for distance and one for near vision. This design helps reduce myopia progression, especially in children with high accommodative lag. Over three years, executive bifocals reduced myopia progression by up to 1.14 diopters compared to single vision lenses. Prismatic bifocals, a special type, may work even better for some children. Executive bifocals outperform single vision lenses in children aged 8-13, making them a strong choice for myopia control treatments.
Progressive Addition Lenses
Progressive addition lenses (PALs) offer a gradual change in lens power from top to bottom. PALs provide modest myopia control, slowing progression by about 0.20 to 0.28 diopters over three years compared to single vision lenses. Children with high accommodative lag or near esophoria may see better results. However, newer spectacle lenses with highly aspherical lenslets and DIMS lenses show greater efficacy for myopic children and adolescents.
Multiple studies show PALs slow myopia progression by 0.14 to 0.59 diopters over 1.5 to 3 years.
The clinical benefit is small for most children, but some subgroups may benefit more.
Single Vision Lenses
Single vision lenses remain the standard correction for myopia, but they do not slow myopia progression. Studies show that children wearing single vision lenses experience more rapid progression and greater axial length growth than those using myopia control treatments. Over four years, children using single vision lenses had up to 0.52 diopters more myopia progression and 0.21 mm more axial length growth than those using advanced spectacle lenses with highly aspherical lenslets.
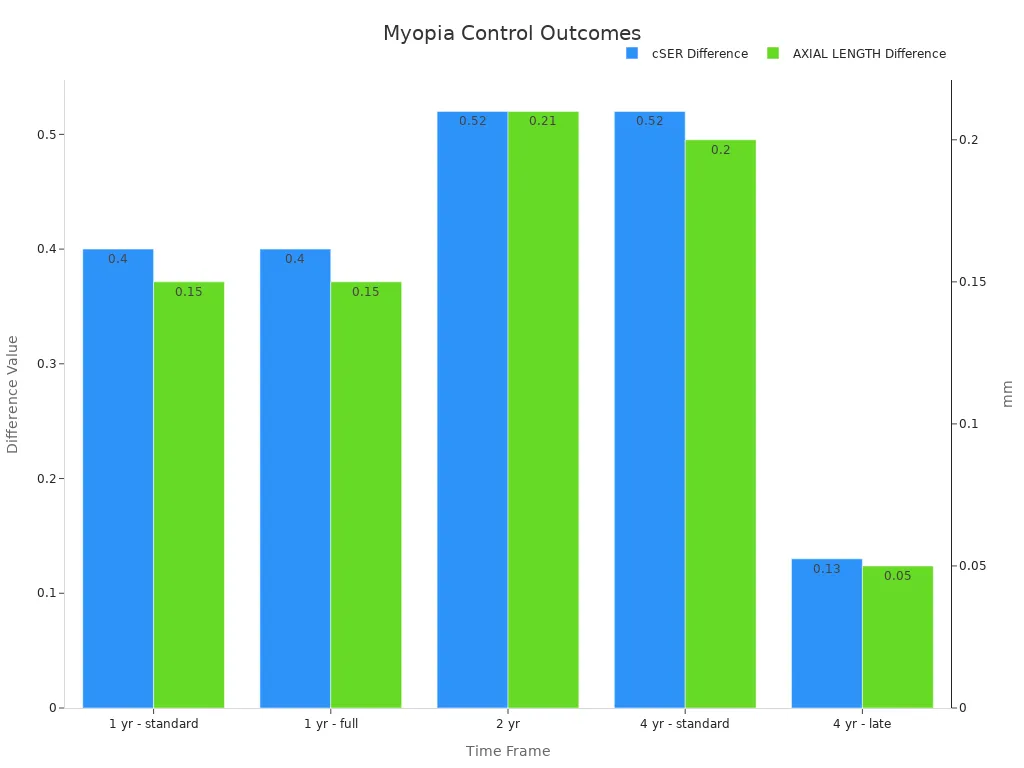
When you compare the effects of different types of spectacle lenses, you see that lenslet-based designs, such as HAL and DIMS, provide the strongest myopia control. The impact of different lens designs is clear: myopic defocus created by these lenses helps protect myopic children and adolescents from rapid progression and future eye health risks.
Lens Comparison

Axial Length Changes
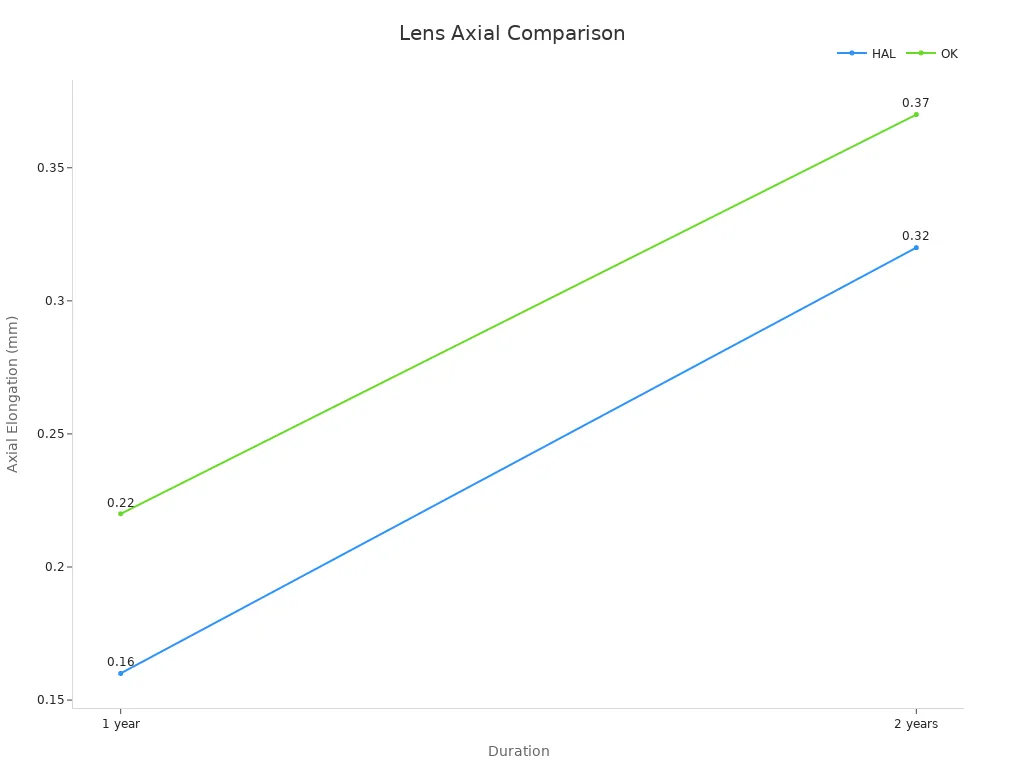
You can measure the success of spectacle lenses for myopia control by looking at axial length changes. Axial length is the distance from the front to the back of the eye. When this length increases too quickly, myopia progression speeds up. Studies show that spectacle lenses with highly aspherical lenslets slow this growth more than other lenses. For example, in younger children, these lenses led to an average axial elongation of 0.16 mm over one year, while orthokeratology lenses showed 0.22 mm. Over two years, the difference remained clear, with 0.32 mm for spectacle lenses with highly aspherical lenslets and 0.37 mm for orthokeratology.
Group |
Lens Type |
Axial Length Elongation (Mean ± SD, mm) |
Duration |
|---|---|---|---|
Younger children (8-10) |
Spectacle lenses with highly aspherical lenslets |
0.16 ± 0.19 |
1 year |
Younger children (8-10) |
Orthokeratology |
0.22 ± 0.17 |
1 year |
Younger children (8-10) |
Spectacle lenses with highly aspherical lenslets |
0.32 ± 0.27 |
2 years |
Younger children (8-10) |
Orthokeratology |
0.37 ± 0.24 |
2 years |
Axial length measurement gives you a reliable way to track myopia progression and lens treatment efficacy.
Refractive Error Changes
You also want to know how spectacle lenses affect refractive error, which measures how much correction your child needs for clear vision. The best spectacle lenses for myopia control show smaller changes in refractive error over time. For example, enhanced efficacy lenses reduced refractive error change by 0.22 diopters compared to single vision lenses at 26 weeks. Dual-focus lenses and enhanced vision lenses also showed improvements, but to a lesser degree.
Lens Group |
Axial Elongation Difference (mm) vs SV |
SECAR Change Difference (D) vs SV |
|---|---|---|
EE |
-0.105 |
0.22 |
EV |
-0.063 |
0.08 |
DF |
-0.056 |
0.12 |
Smaller refractive error changes mean slower myopia progression and better long-term myopia control.
Peripheral Defocus Mechanism
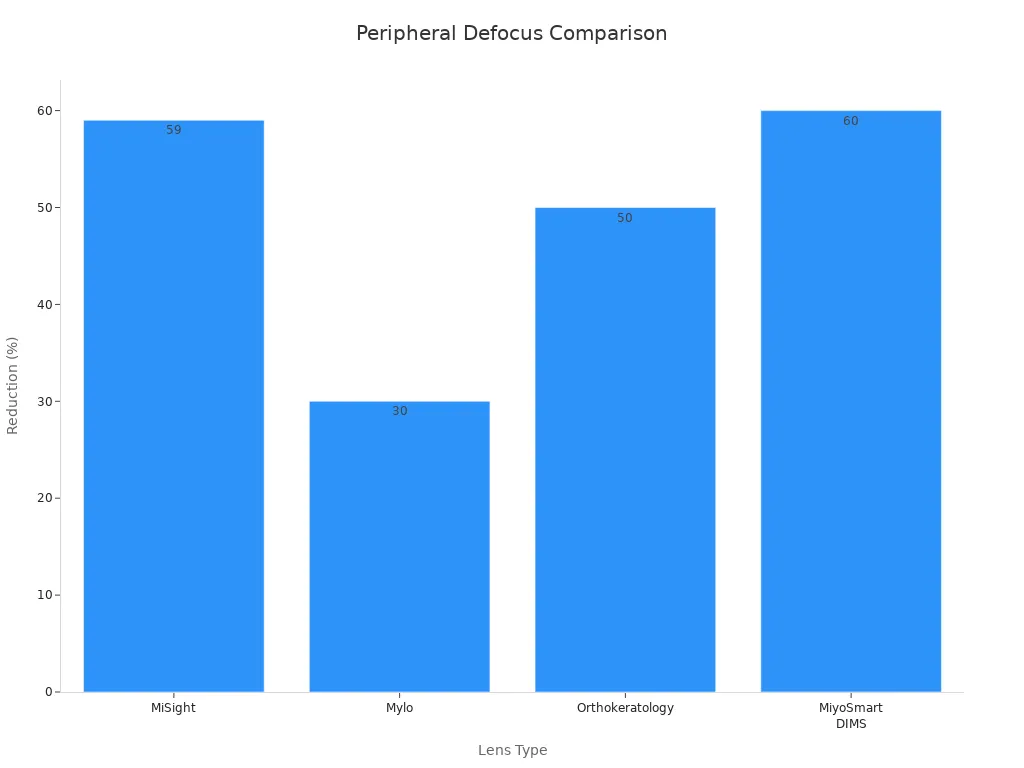
Spectacle lenses with myopic defocus technology change how light focuses on the retina. These lenses create a special blur in the eye’s periphery, which tells the eye to slow its growth. This mechanism is key for myopia control. Lenses like DIMS and Stellest use this approach and show about 60% effectiveness in slowing myopia progression. Orthokeratology and MiSight contact lenses also use peripheral defocus and show strong results.
Lens Type |
Mechanism |
Myopia Progression Reduction |
|---|---|---|
DIMS (MiyoSmart) |
Peripheral defocus annular zones |
~60% |
Stellest |
Aspheric lenslets creating myopic defocus |
~60% |
Orthokeratology |
Corneal shape-induced peripheral defocus |
~50% |
MiSight |
Dual-focus (contact lens) |
59% |
Myopic defocus is a proven way to slow myopia progression and protect your child’s vision.
Choosing the Right Spectacles for Myopia
Age and Severity
You should always consider your child’s age and the severity of their myopia when selecting spectacles. Younger children often experience faster myopia progression, which means you may need to update their prescription more frequently. For example, children aged 8 to 13 can have a progression rate of about -0.31 diopters per year, while adolescents and young adults see much slower changes. Myopia usually stabilizes between ages 14 and 17, so older adolescents require fewer prescription changes.
Age Group / Factor |
Myopia Progression Rate |
Stabilization Age |
Impact on Spectacle Performance |
|---|---|---|---|
Children (8-13 yrs) |
~-0.31 D/year |
N/A |
Frequent updates needed |
Adolescents (20-22 yrs) |
~-0.10 D/year |
14.4-16.7 yrs |
Slower progression, stable Rx |
Severity at Stabilization |
Mean -4.87 D (±2.01) |
N/A |
Higher risk, more complex care |
Children with higher myopia face greater risks of eye complications and may need specialized lenses. Severe myopia can also increase the cost and complexity of management. You should discuss these factors with your eye care provider to find the best treatment options.
Binocular Vision Status
Before starting any myopia control strategy, you need to check your child’s binocular vision. Many myopic children show issues like high accommodative lag or near esophoria. These problems can affect how well certain treatment options work. For example:
Children with near esophoria progress faster with single vision lenses than with progressive addition lenses.
Multifocal and dual-focus lenses may reduce accommodative response and cause exophoric shifts.
Orthokeratology can improve accommodative function but may reduce fusional vergence range.
Addressing binocular vision problems can improve comfort, reading, and even the effectiveness of myopia management.
You should ask your eye care professional to test for binocular vision issues before choosing a lens. Sometimes, vision therapy or special lens designs can help manage these problems.
Lifestyle and Compliance
Your child’s daily activities and willingness to wear spectacles play a big role in the success of any myopia control strategy. Active adolescents may prefer lightweight or impact-resistant lenses. Children who spend a lot of time reading or using screens may benefit from lenses that address accommodative lag. Severe myopia often requires thinner, lighter lenses for comfort and better appearance, which can improve compliance.
🟢 Tip: Involve your child in the decision-making process. When children help choose their frames and understand the benefits of their treatment options, they are more likely to wear their spectacles consistently.
You should also consider how often you can visit the eye doctor for follow-up. Frequent check-ups help track myopia progression and adjust treatment strategies as needed. Reliable statistical measures, such as mean bias and mean absolute error, help your provider monitor changes in axial length and refractive error, ensuring the chosen management plan works well.
Recommendations
For Parents
You want the best for your child’s eyes. Choosing the right spectacles for myopia can feel overwhelming, but you have strong options. Modern spectacle lenses, like those with DIMS or highly aspherical lenslet technology, show high effectiveness in slowing myopia progression. These lenses can reduce the risk of future eye problems and help your child see clearly.
Here is a quick comparison of popular spectacle lenses for children:
Spectacle Lens Type |
Age Range (years) |
Myopia Progression Reduction (%) |
Axial Elongation Reduction (%) |
Notes |
|---|---|---|---|---|
Progressive Addition Lenses (PALs) |
~6-12 |
Modest, not always significant |
N/A |
Best for children with focusing problems |
Myovision (Peripheral Plus) |
6-12 |
20% |
Not significant |
Studied in Chinese children |
Executive Bifocals (+1.50D add ± 3D prism) |
N/A |
Significant vs single vision |
N/A |
Greater effect with prism in some children |
MiYOSMART (DIMS technology) |
N/A |
62% |
Multiple focal zones for better control |
|
Highly Aspherical Lens Technology (HALT) |
N/A |
60% (1st year) |
28% (1st year) |
Uses aspherical lenslets in rings |
Stellest Lenses |
N/A |
Equivalent to 1.75 D saved |
N/A |
Available in sun tints |
SightGlass Vision (DOT) |
N/A |
Significant slowing |
4-year data confirms sustained effect |
🟢 Tip: Ask your eye doctor about these lens types. Some lenses work better for certain ages or vision needs.
You should also know that spectacle lenses now offer results similar to contact lenses for myopia control. If your child feels nervous about contacts or eye drops, spectacles are a safe and effective choice. Some children benefit from combining spectacles with other treatments, like atropine drops, especially if they have binocular vision issues.
Keep these points in mind:
Schedule regular eye exams to track your child’s progress.
Encourage your child to wear their spectacles every day.
Support healthy habits, like outdoor play and limited screen time.
Talk to your eye care provider about any changes in vision or comfort.
Long-term monitoring of myopia progression helps you and your doctor adjust the treatment plan as your child grows. Early action and consistent follow-up can make a big difference in your child’s eye health.
For Clinicians
You play a key role in guiding families through myopia management. Recent clinical trials highlight the importance of matching lens type to patient characteristics. Here are some practical guidelines:
New spectacle lens designs, such as DIMS, HALT, and DOT, show statistically significant slowing of myopia progression and axial elongation in randomized controlled trials.
Progressive addition lenses (PALs) provide a modest benefit, especially for children with accommodative lag or esophoria. The effect may diminish after 6-12 months.
Consider binocular vision status before recommending a lens. PALs may help children with focusing problems, while lenslet-based designs suit a wider range of patients.
Patient-specific factors, such as age, baseline refractive error, astigmatism, and lifestyle, should guide lens selection.
Astigmatism correction matters. Orthokeratology works well for astigmatism over 0.75D, while soft multifocal lenses suit lower levels.
Follow-up schedules should match the treatment type. For example, multifocal soft lenses need visits at 1 week, 1 month, and 6 months. Orthokeratology requires more frequent early visits.
Wearing time impacts efficacy. Multifocal soft lenses should be worn 5-8 hours per day. Ortho-k lenses require at least 8 hours per night.
Combine optical or pharmacological treatments with lifestyle advice for the best results.
📋 Note: The most effective myopia control lenses reduce axial length progression by about 50% compared to single vision controls. Always monitor for side effects and adjust the plan as needed.
You should encourage families to return for regular check-ups. Long-term monitoring of myopia progression ensures that you can respond quickly to changes and maintain effective management.
You have strong options for managing myopia in children. Next-generation spectacle lenses, such as those with highly aspherical lenslets, show the greatest reduction in myopia progression and axial elongation. Clinical studies highlight the need for individualized lens selection based on age, eye health, and lifestyle. Always consult your eye care professional for tailored advice. Take action early to protect your child’s vision and support long-term eye health.
FAQ
What age should my child start wearing myopia control spectacles?
You can start myopia control spectacles as soon as your child is diagnosed with myopia. Early treatment works best. Children as young as six can benefit from these lenses. Your eye doctor will help you decide the right time.
How often should my child have eye exams when using myopia control lenses?
You should schedule eye exams every six months. Regular check-ups help track your child’s progress. Your doctor can adjust the prescription if needed. Early detection of changes keeps your child’s eyes healthy.
Are myopia control spectacles safe for long-term use?
Yes, myopia control spectacles are safe for daily and long-term use. Studies show no harmful effects from wearing these lenses. You should encourage your child to wear them as recommended for the best results.
Can my child switch from single vision lenses to myopia control lenses?
You can switch your child from single vision lenses to myopia control lenses at any time. The change helps slow myopia progression. Your eye care provider will guide you through the process and answer your questions.




